Need a kidney transplant? You better be poor according to new DEI proposed rules
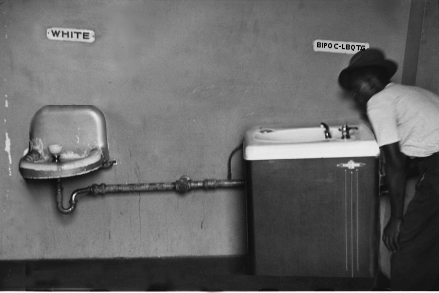
The Biden administration: still dedicated to segregation!
“Segregation today, segregation tomorrow, segregation forever!” According to new rules proposed by the Biden administration “to root our racial bias,” a pilot program will favor low-income patients in providing them kidney transplants.
The proposal, which Becerra’s agency announced on May 8, would place 90 of the nation’s 257 transplant hospitals into a pilot program that uses an annual point system to grade participants. Under the system, a successful kidney transplant counts as one point. A transplant furnished to a low-income patient, however, counts as 1.2 points thanks to a “health equity performance adjustment,” thus incentivizing the hospitals to prioritize such patients. At the end of each year, those points are applied to a transplant quota. Hospitals that meet their quota receive as much as $8,000 per transplant; those that don’t may have to pay up to $2,000 per transplant.
While the proposal uses income to categorize patients rather than race, Becerra made clear that the scoring system is meant to address racial concerns. In his statement announcing the proposal, he touted the Biden administration’s “concrete steps to remove racial bias … in the transplant process.”
This is clearly aimed at favoring minorities over whites, and we know this because the administration specifically decided to opt out of considering “rural” a low-income qualification. Since a large percentage of low-income whites live in rural communities, this decision guarantees that the rules will favor minorities.
Regardless, by bringing the income of patients into the equation the Biden administration is guaranteed to poison medical decisions, which should be decided solely by the health concerns of each patient, not by outside political factors.
The proposal itself [pdf] is 381 pages long, incredibly dense and obtuse in its language, and complex beyond belief. It is guaranteed to cause administrative headaches and additional costs to the hospitals involved, which is also guaranteed to negatively impact the ability of those hospitals to care for patients. In other words, more overhead and larger administrative staffs, and less money for doctors and nurses.
The plan does not list the 90 hospitals that will participate in this pilot program. It is critical that this list be revealed as soon as possible, so that every sick person nationwide who is not poor and who might need a kidney can avoid such places. It will also be good for the general public to know which hospitals are willing to go along with such madness, as it will reveal their priorities are focused not with patient care but in implementing the left’s Marxist DEI agenda.
The proposal, if implemented, is scheduled to go into effect in January 2025. Thus, this becomes another reason to vote against Biden in the November election. His defeat will almost certainly cancel this entire idiocy.
On Christmas Eve 1968 three Americans became the first humans to visit another world. What they did to celebrate was unexpected and profound, and will be remembered throughout all human history. Genesis: the Story of Apollo 8, Robert Zimmerman's classic history of humanity's first journey to another world, tells that story, and it is now available as both an ebook and an audiobook, both with a foreword by Valerie Anders and a new introduction by Robert Zimmerman.
The print edition can be purchased at Amazon or from any other book seller. If you want an autographed copy the price is $60 for the hardback and $45 for the paperback, plus $8 shipping for each. Go here for purchasing details. The ebook is available everywhere for $5.99 (before discount) at amazon, or direct from my ebook publisher, ebookit. If you buy it from ebookit you don't support the big tech companies and the author gets a bigger cut much sooner.
The audiobook is also available at all these vendors, and is also free with a 30-day trial membership to Audible.
"Not simply about one mission, [Genesis] is also the history of America's quest for the moon... Zimmerman has done a masterful job of tying disparate events together into a solid account of one of America's greatest human triumphs."--San Antonio Express-News
“The proposal itself is incredibly dense and obtuse in its language, and complex beyond belief.” Boy, that’s for sure an understatement.
Reading all of the papers by the Bernoulli family in the 17th-18th centuries would be less involved. Nancy Pelosi even said “Give me that Obamacare Law any day over this dang thing”.
I read some and scanned all of this monster proposal. A good middle-school English student could have simplified it to 20 pages. But that’s only if you want clarity and no governmentese.
There is no table of contents, and no index. But “definitions” are on p. 312-324.
Page 8 makes MANDATORY that 90 hospitals participate. The Organ Procurement and Transplantation Network (OPTN) lists only 248 transplant centers [see https://optn.transplant.hrsa.gov/about%5D, not 257.
P 100-101 – Point system of 60-20-20 for achievement, efficiency, and quality domains. See p. 329-332, 332-335, 335-340 respectively for how these domains are to be calculated and points awarded. These are complicated algorithms.
p 116-117 – how they chose the 1.2 multiplier instead of 1.1.
p. 167-173 for calculating payments to hospitals. “Significant weight should be given to performance in the achievement domain,” At least they seem to be valuing achievement.
p. 194 – Net worth and racial disparities tip the present transplantees toward the wealthy and white folks. But we can’t have that now can we?
p. 245 – shows an adder of +$103 for part B-ID benefit Medicare premium if MFJ MAGI > $206K. I must not be understanding the “-ID” part, because the part B (no -ID) adder is $244.60 on the SS website for MFJ-MAGI > $206K.
p. 294-298 – shows their calculation of the estimated costs & savings involved to the hospitals, the kidney recipient, and Medicare.
The phrase “attributed patient” was used 393 times. “Attribution” used 147 times. “Health equity” 105 times. See “Definitions” p. 312+.
The word ‘racist’ does not appear anywhere in the proposal. Whew – at least the writers aren’t bigots. But ‘racial’ appears 25 times.
I suspect that they are grossly underestimating the increased administrative costs to the hospitals. They don’t seem to include the many meetings of the boards of directors to discuss how a hospital can make money conforming to another regulation.
Sorry – delete the %5D from the end of the OPTN website.
This year my tech company went with a new health insurance company and all the doctors in their network accepting new patients are ESL women immigrants primarily from China and India.
“I suspect that they are grossly underestimating the increased administrative costs to the hospitals.” – Don C.
“Regulatory Burden Under Biden Soars to $1.6 Trillion and 292 Million Paperwork Hours”
https://www.theepochtimes.com/us/regulatory-burden-under-biden-soars-to-1-6-trillion-and-292-million-paperwork-hours-5656858?utm_source=partner&utm_campaign=TheLibertyDaily
I’ll state the obvious to Americans – they have no right to do that. Too bad there are to few Americans left in the country. This kind of garbage needs to be defunded.
If it’s any consolation a whistleblower claims that half of UCLA medical students now fail basic tests of medical comptence . So it isn’t like they will be anyone available to do kidney transplants in DIE America.
I hope they do know that there are numerically more white poor than black poor just by the numbers. Unless they go per capita and that would be racist.
I have for years thought that the old racist civil war era southern idea that even 1 percent black is black should be cast aside. The new racists both black and white are still using it.
I think that if people still want to use some racial category or metric to apply benefits to then I think we should set a genetic majority measurement and limit. Genetics does not go by how you outwardly look.
The only groups that should be allowed to have a lower than genetic majority should be native tribes. They all tend to have different requirements to become members. At least one will only take documented evidence and some will take a genetic test as low as 5%.
I believe that the simple fact that knowing your genetic heritage will reduce the vast majority of racism in America.